

Most practices respond to claim denials instead of preventing them, and that reactive default is expensive. According to MGMA survey data, roughly 26% of providers report that approximately 10% of their denials stem from inaccurate or incomplete data collected at intake. Those are not complex payer disputes. Those are administrative errors that never should have reached a payer in the first place. A structured denial prevention approach eliminates most of them before submission.
The financial cost of that backward approach compounds fast. Every denied claim requires staff time to review and rework, and some never get appealed at all. Revenue quietly disappears. Because the team is always working the denial queue, nobody has bandwidth to fix the upstream processes generating the denials in the first place.
This article answers one core question: what is the actual difference between denial prevention and denial management, and why does that distinction matter for your bottom line? Many case studies and benchmarking reports show that practices partnering with prevention-focused billing teams see meaningful gains over those running purely reactive appeals workflows. The gap is real. Here is how to understand it, measure it, and close it.
What denial prevention and denial management actually mean
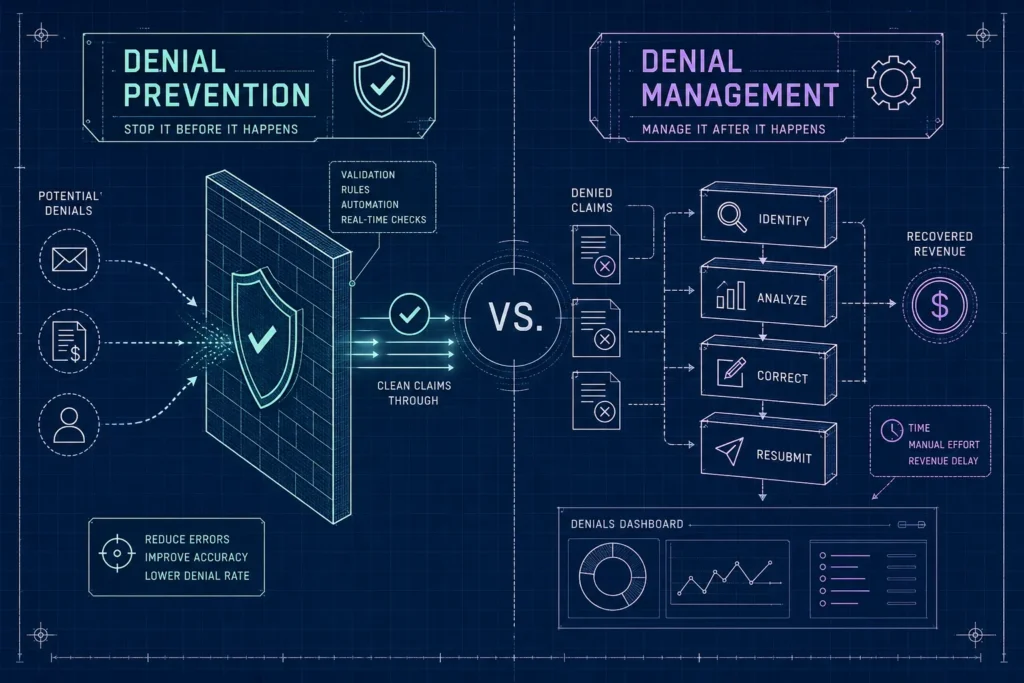
Prevention stops denials before a claim leaves your office
Denial prevention is the upstream set of processes designed to eliminate billing errors, documentation gaps, and authorization failures before a claim is ever submitted. It includes eligibility verification, pre-authorization checks, coding accuracy reviews, and claims scrubbing. The goal is a clean claim on the first pass, meaning the payer accepts it without requesting corrections or additional information.
This is not a passive process. It requires structured workflows, assigned ownership, and technology that flags problems before submission rather than after. A clean claim rate above 95% is the benchmark for practices doing this well. Industry benchmarks identify rates below 90% as a warning threshold; if yours is in that range, you have a prevention gap that is likely costing you money every month.
Management is damage control after the payer says no
Denial management is the reactive workflow that kicks in after a claim is denied. It means reviewing the denial reason, filing appeals, gathering documentation, and resubmitting. It is necessary, and some portion of denied revenue does get recovered through this process. But it does not fix the root problem, and it is not cheap.
Per MGMA and HFMA benchmarks, reworking a single denied claim costs anywhere from $25 to over $180 depending on complexity and payer, with a commonly referenced administrative average of around $57 per claim. Multiply that by a denial rate of 8 to 12% across hundreds of monthly claims and the labor cost becomes significant fast. That math does not improve until you address the upstream causes.
Why this distinction determines your revenue cycle health
Practices that invest heavily in management but underinvest in prevention are on a treadmill. They recover some denied revenue through appeals, but new denials keep arriving because the root causes were never addressed. The distinction goes beyond semantics, it is a strategic choice with real financial consequences. Your revenue cycle health reflects which side of that choice you are on. Consider a mid-sized behavioral health group spending 15 hours a week on appeals: that same time, redirected to front-end verification, would likely eliminate more revenue loss than the appeals ever recover.
Why reactive denial management costs more than most practices realize
Revenue that never comes back
Not all denied claims get appealed, and not all appeals succeed. Denial write-offs, revenue permanently lost to uncontested or unsuccessfully appealed denials, directly reduce net patient service revenue. Practices with high denial rates in specialties like behavioral health, which runs 8 to 15% (see average claim denial rates by specialty), or physical therapy, which runs 7 to 12%, are particularly exposed to this kind of ongoing revenue leakage. Those numbers represent real dollars gone for good.
The hidden opportunity cost
Every hour a billing team spends on denial management is an hour not spent on proactive verification, coding review, or payer policy updates. Reactive teams stay stuck in the same cycle because they never have the bandwidth to fix the upstream issues causing the denials. It is a well-documented operational pattern in revenue cycle management (RCM): when staff are consumed by denial queues, process improvement stalls indefinitely. Recent healthcare claim denials statistics underscore how widespread these denial-related burdens are.
The four pillars of a strong denial prevention strategy
Clean claim submission starts at patient registration
The first line of defense is accurate patient demographic and insurance data collected at intake. Eligibility verification, coordination of benefits confirmation, and coverage checks before the appointment eliminate a large share of administrative denials. A 2023 case study published by a healthcare technology vendor found that automated front-end eligibility checks helped one health system recover $1.16M in revenue in just six months while reclaiming 46,000 staff hours. That return came entirely from fixing the front end, before a single claim was submitted.
Pre-authorization verification cannot be an afterthought
Missing or incorrect prior authorization is one of the most consistently cited denial causes across all payer types. Before any service is rendered, the practice needs to confirm whether the payer requires authorization, obtain it, document the approval number, and attach it to the claim. A single missed authorization can trigger a denial that takes weeks to appeal and may never be overturned. In 2026, with payer prior authorization requirements continuing to tighten, this step is not optional.
Coding accuracy is where clinical and billing teams intersect
Incorrect CPT or ICD-10 codes, unmatched diagnosis-procedure pairings, and missing modifiers generate preventable denials. Regular coding audits, coder education on payer-specific policies, and clinical documentation improvement initiatives all reduce this category. Coding accuracy is especially critical in high-scrutiny specialties like ABA therapy and behavioral health, where payer documentation requirements are unusually strict and progress-note gaps are a frequent trigger for both initial denials and post-payment audits.
Claims scrubbing catches errors before submission
A claims scrubbing step, whether built into your billing software or performed by your billing team, runs each claim through a set of edits that flag incomplete fields, invalid payer data, missing authorizations, and other preventable errors before the claim reaches the payer. This front-end filter is one of the highest-return investments in your revenue cycle. It turns errors into corrections rather than denials.
Payer rule monitoring: the prevention step most practices skip
Payer policies change more often than most teams track
Commercial payers update their coverage policies, prior authorization requirements, and medical necessity criteria on an ongoing basis, with formal internal reviews often occurring at least annually. A billing process that was compliant six months ago may generate medical billing denials today because a payer quietly changed its documentation requirements for a CPT code your practice bills frequently. Practices without a formal process for monitoring payer updates are perpetually caught off guard.
How to build a practical payer intelligence process
Assign ownership of payer monitoring to a specific team member or billing partner. Subscribe to payer bulletins and policy update notifications. Track changes to prior authorization requirements for your top five payers by claim volume. When a payer updates its rules for a code your practice uses frequently, that update needs to reach your coders and front-desk staff before the next claims batch goes out.
The denial impact of ignoring policy changes
Practices that do not track payer policy updates tend to see clusters of denials with similar reason codes appearing suddenly, usually traced back to a policy change no one caught. Research into denial root causes consistently identifies policy-change-related denials as largely preventable with proper monitoring in place. They represent one of the clearest cases where a proactive process would have protected revenue that instead requires time-consuming appeals to recover. For behavioral health and physical therapy providers especially, where payer scrutiny is already elevated, missing a policy update is a costly gap.
KPIs that tell you whether your prevention efforts are working
Clean claim rate is your primary leading indicator
Clean claim rate measures the percentage of claims accepted by payers on first submission without corrections or additional information required. This is the most direct measure of how well your front-end prevention processes are performing within your revenue cycle management (RCM) program. Top-performing practices achieve clean claim rates above 95%, with high-performers reaching 96 to 98%. If yours is below 90%, the industry warning threshold identified by HFMA, that gap represents a concrete denial prevention opportunity with a measurable financial upside.
Denial rate by reason code reveals where to focus
Tracking denial rate by reason code, broken down by payer, provider, or service line, turns a general denial rate into a root-cause roadmap. If your top denial reason is missing prior authorization, you know exactly where to fix your process. If it is invalid procedure code, the problem is upstream in coding or charge capture. A general denial rate number is a scoreboard; reason-code analysis is the game film.
The financial KPIs leadership needs to see
Denial write-offs as a percentage of net patient service revenue and initial denial rate by both dollar and volume give leadership a clear picture of how much revenue is at risk and how much is being permanently lost. Appeal overturn rate rounds out the picture by showing whether denial management is successfully recovering revenue when prevention falls short. Per HFMA guidance, practices targeting strong financial performance typically aim to keep denial write-offs below 1% of net patient service revenue, a threshold that becomes achievable when denial prevention strategies are doing the heavy lifting upstream.
When outsourcing denial prevention beats building it in-house
The real cost of in-house billing for small practices
Hiring, training, and retaining a capable in-house billing team with genuine denial prevention expertise is expensive. A single experienced biller with RCM knowledge can cost $45,000 to $65,000 per year in salary alone, before benefits, training, and software. Small practices with fewer than six providers often end up with generalist staff handling claims reactively rather than running the structured prevention workflows that actually reduce denial rates. The overhead is high and the specialized expertise is hard to sustain.
What a prevention-focused billing partner does differently
A billing service built around denial prevention does not just submit claims. It verifies eligibility before every appointment, flags missing authorizations before claims go out, monitors payer policy changes on your behalf, and runs claims scrubbing as a standard part of every submission. The difference is not just efficiency, it is whether your revenue cycle is designed to prevent revenue loss or chase it down after the fact. Those are fundamentally different operating models.
WeBill Health is built for practices that can’t afford high denial rates
WeBill Health works specifically with small and mid-sized practices in high-denial specialties: behavioral health, physical therapy, and ABA therapy. The approach centers on proactive denial prevention, clean submissions, pre-authorization support, specialty-specific coding expertise, and payer rule monitoring built into every engagement. Practices that have shifted from in-house reactive billing to a prevention-first model typically report lower denial rates and reduced appeals overhead; WeBill Health’s engagements are structured to deliver that same outcome. If your current billing setup is generating appeals backlogs instead of clean claims, that gap is worth a conversation.
Protecting revenue upstream is always cheaper than chasing it downstream
The difference between denial prevention and denial management is the difference between protecting revenue before it disappears and scrambling to recover it after. Both are necessary parts of a complete revenue cycle, but practices with the healthiest cash flow invest upstream: in eligibility checks, prior authorization verification, coding accuracy, claims scrubbing, and payer monitoring. They use denial management as a safety net, not a primary strategy.
If building that kind of prevention-first infrastructure in-house is not realistic for your practice right now, outsourcing to a billing partner designed specifically around denial prevention strategies is often the more cost-effective path. Your internal staff can focus on what actually moves the needle instead of working denial queues that should not exist in the first place.
Start with your clean claim rate and your top five denial reason codes. Those two data points will tell you exactly where revenue is leaking. Everything else follows from there. Contact WeBill Health for a denial prevention audit and find out what a prevention-first revenue cycle could mean for your practice.


















